For each VAG signal graphical illustrations are provided in the following order:
Note: After the graphical illustrations, sounds are provided for auditory display. For auditory display of VAG signals the playback rate has to be 2 kHz.
| Project Summary |
|
Human knee joint vibration or sound signals, also known as vibroarthrographic (VAG) signals, emitted during active movement of the leg are expected to be associated with pathological conditions (such as arthritis) of the articular cartilage of the knee. The main motivating factors for using VAG as a noninvasive diagnostic tool for monitoring cartilage disorders are: inexpensive data acquisition setup, inability of current imaging techniques to capture intricate cartilage changes, and advances in digital signal processing techniques. VAG signals are nonstationary (i.e., the signal statistics/spectral contents vary with time) in nature, which arises due to the fact that different joint surfaces come in contact during movement, and the nature and quality of the joint surfaces coming in contact may not be same from one position of the knee to the next. Hence both intra- and inter-subject variability of signal characteristics are expected. In our initial studies on VAG, common signal processing techniques such as the Fourier transform or autoregressive (AR) modeling were applied to VAG signals by assuming the signal to be either stationary or by segmenting the signal into quasi-stationary parts. Although the above methods addressed nonstationarity to some extent by using robust adaptive segmentation algorithms, there was a difficulty in labeling individual segments as normal or abnormal. This is because accurate estimation of the joint angle corresponding to pathology as observed during auscultation or arthroscopy could not be achieved. This problem could be obviated by using nonstationary signal analysis tools such as time-frequency (TF) transforms. TF transforms give time-varying spectral information as a two-dimensional (2D) representation in time and frequency, and are suitable for tracking the nonstationary behavior of signals. High TF resolution and interference-free TF distributions (TFDs) of VAG signals were obtained in our work by using the matching pursuit method. Adaptive TFD can be constructed by optimizing the matching pursuit TFD with constraints of desired marginals. TF features such as instantaneous energy, instantaneous energy spread, instantaneous frequency, and instantaneous frequency spread were extracted from the adaptive TFDs. Pattern classification of VAG signal features indicate accuracy up to 86% in screening abnormal knees from normal knees, and has particularly shown high sensitivity in screening patellofemoral articular cartilage disorders such as chondromalacia patella. TF parameters based on frequency have contributed significantly towards accurate screening of VAG signals. This gives motivation to look for frequency modulated (FM) components in the TF plane. Abnormal knees have rougher cartilage surfaces than normal knees, and hence the VAG signals emitted by abnormal knees should have different frequency dynamics as compared with VAG signals of normal knees. Hough and Radon transforms can detect lines and curves in an image. The FM dynamics of a signal are represented as lines and curves in its TFD. Hough and Radon transforms of TFDs of simulated signals have provided good results in detecting FM components in noisy environments. This technique has been extended to TFDs of real VAG signals for extraction of FM patterns/signatures which could aid in better screening and help us understand how the movement of knee affects VAG patterns. Direct auscultation of knee joints has been a traditional mode of diagnosis. Computer-aided auscultation using auditory display procedures has been developed in our lab. A pilot study on auditory display of VAG signals has shown promising potential with a sensitivity of 83% in screening abnormal knees, although at the expense of a decrease in specificity. The techniques developed are being incorporated in a diagnostic workstation being prototyped. |
| Illustrations |
|
For each VAG signal graphical illustrations are provided in the following order: Note: After the graphical illustrations, sounds are provided for auditory display. For auditory display of VAG signals the playback rate has to be 2 kHz. |
| Normal VAG1 |
|
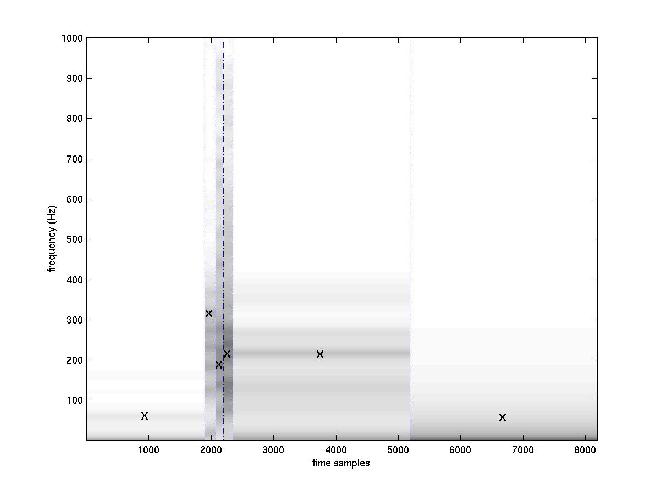
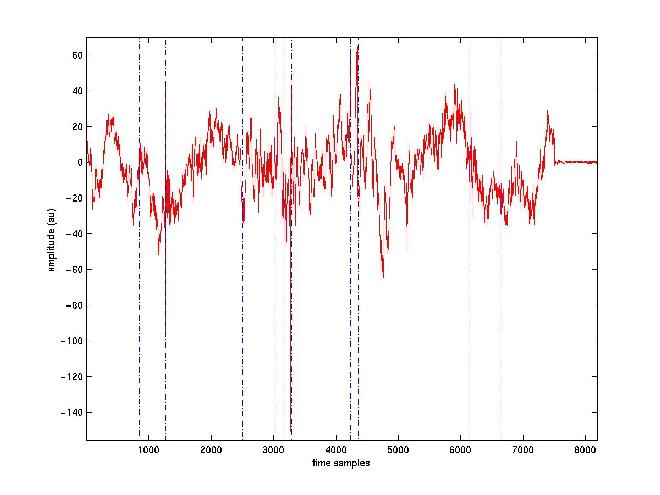
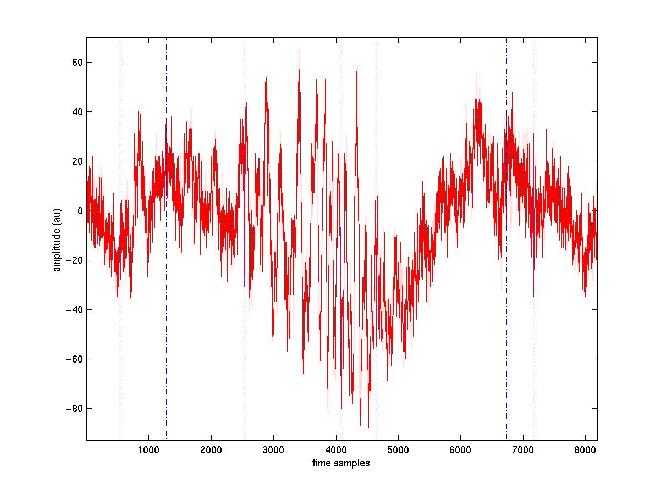 VAG signal obtained from a normal silent knee. Dotted vertical lines denote the adaptive segment boundaries. Please note that because of the low resolution of the image the dotted lines may not be visible in some cases.
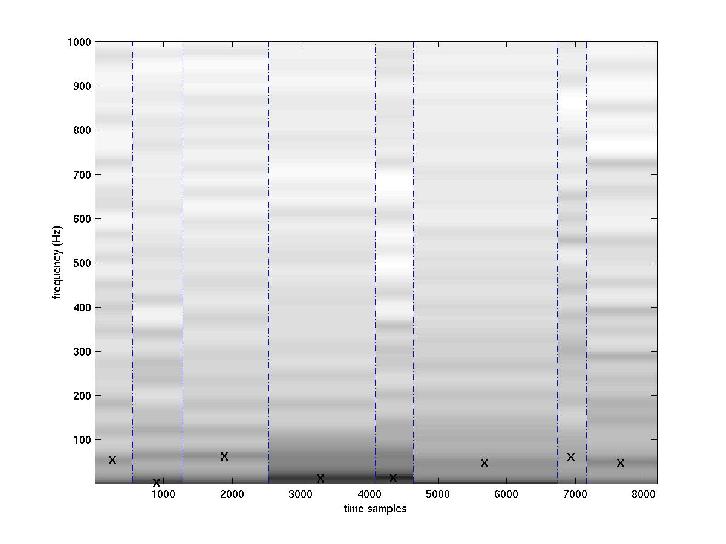 AR spectra in a time-frequency representation. X's denote the most dominant pole in each segment.
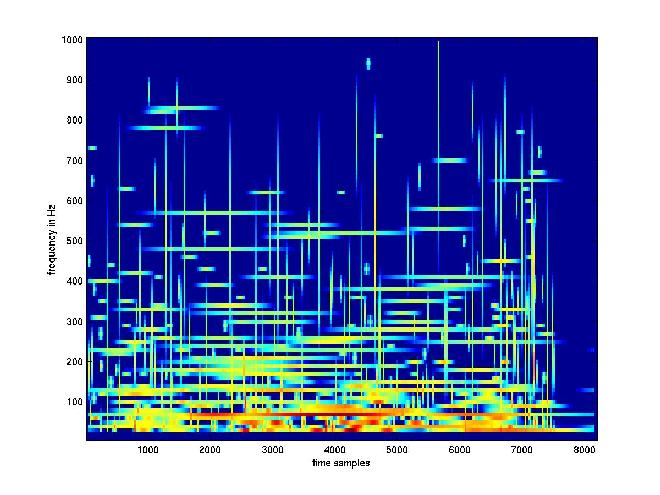 Adaptive time-frequency representation.
Auditory Display: Original sound (4 secs) (wav format for PCs) (au format for SUNs) |
| Normal VAG 2 |
|
VAG signal obtained from a normal noisy knee.
 AR spectra in a time-frequency representation. X's denote the most dominant pole in each segment.
 Adaptive time-frequency representation.
Auditory Display: Original sound (4 secs) (wav format for PCs) (au format for SUNs) |
| Abnormal VAG 1 |
|
VAG signal obtained from an abnormal knee with chondromalcia grade II.
 AR spectra in a time-frequency representation. X's denote the most dominant pole in each segment.
 Adaptive time-frequency representation.
Auditory Display: Original sound (4 secs) (wav format for PCs) (au format for SUNs) |
| Abnormal VAG 2 |
|
VAG signal obtained from a abnormal knee with chondromalacia grade IV.
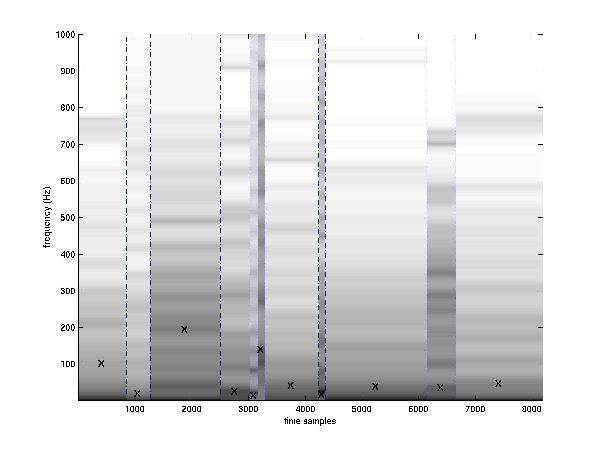 AR spectra in a time-frequency representation. X's denote the most dominant pole in each segment.
 Adaptive time-frequency representation.
Auditory Display: Original sound (4 secs) (wav format for PCs) (au format for SUNs) |
| Illustrations: Muscle Contraction Interference Removal |
|
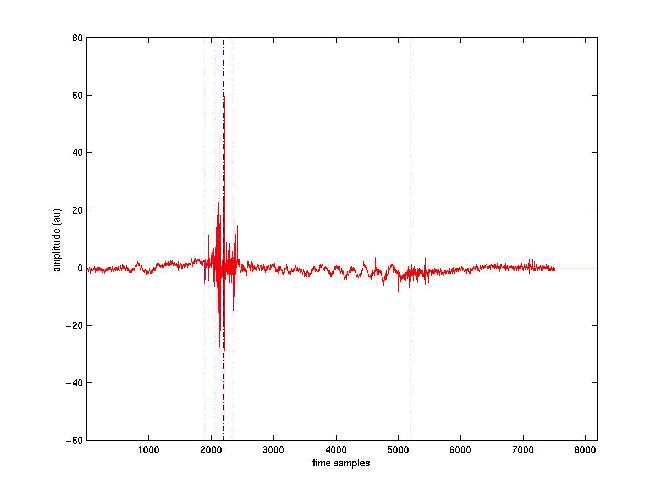
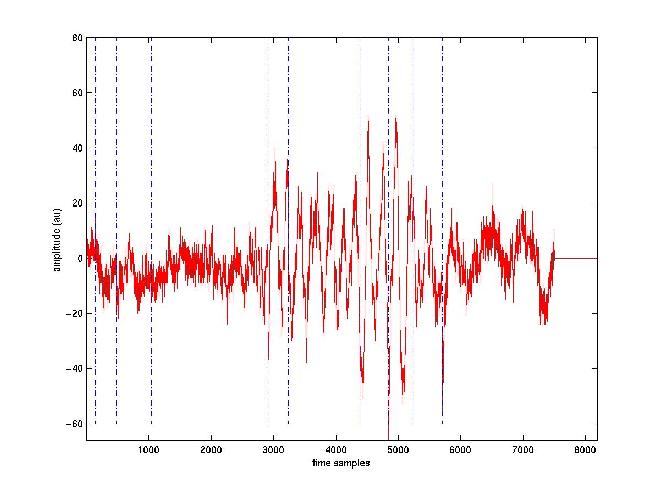
VAG signals emitted from knee joints due to the contact and rubbing of articular cartilage surfaces during normal movement of the knee may bear diagnostic information about the knee joint. As VAG signals are recorded during dynamic movement while flexing and extending the knee, muscle contraction forces play a vital role (especially during extension) in knee movement. Signals related to the muscle contraction forces may interfere with the primary VAG signal of clinical interest recorded at the mid-patella position, and are termed as muscle contraction interference (MCI). To facilitate accurate analysis of VAG signals, MCI has to be filtered from the primary VAG signal. Due to the random behavior of MCI and VAG signals, conventional filtering techniques are not appropriate for MCI cancellation. MCI during dynamic movement of the knee has to be adaptively filtered for efficient removal from the VAG signals. Adaptive filters based on LMS and RLS algorithms were designed for MCI removal. The following figures graphically illustrate the MCI removal results.
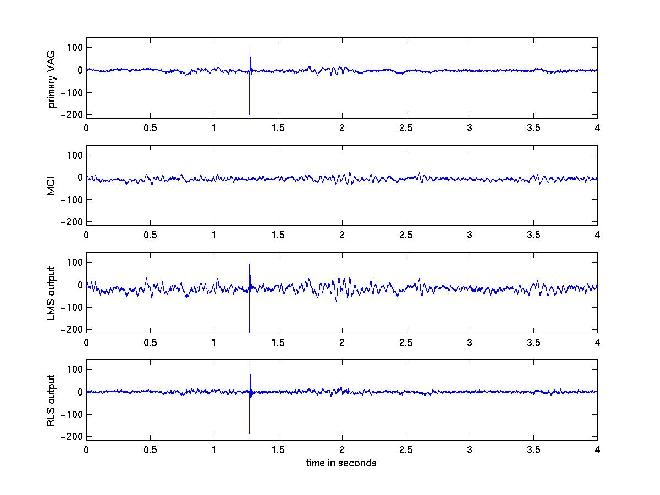 Graphs of MCI removal. Time-domain illustration.
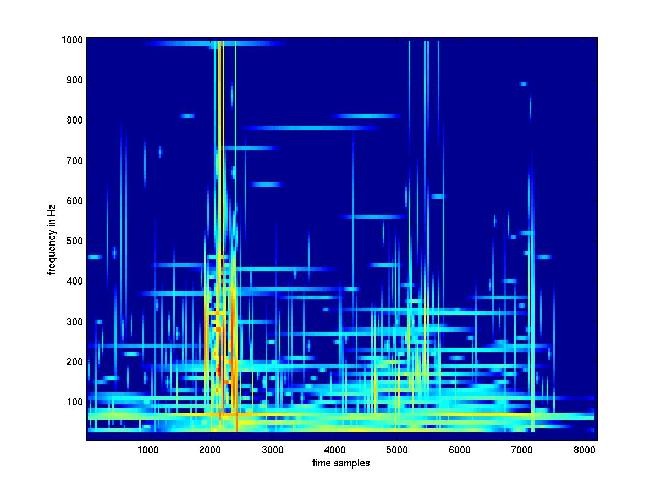
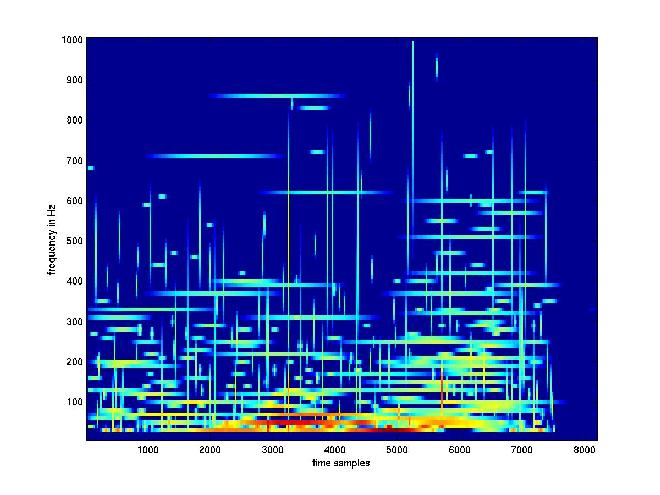
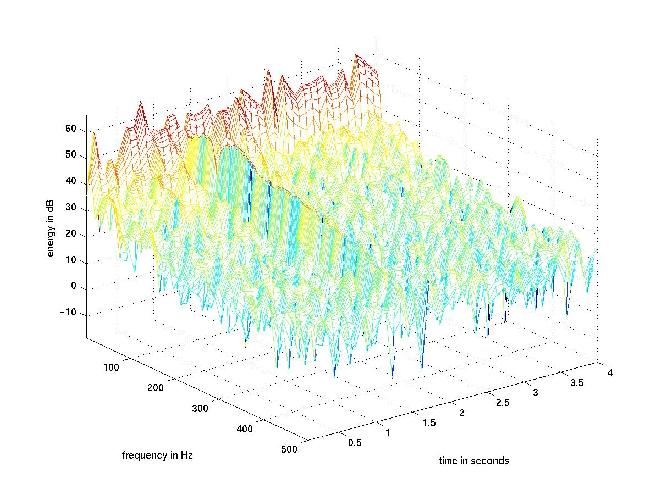 TFD of the original VAG signal without MCI filtering.
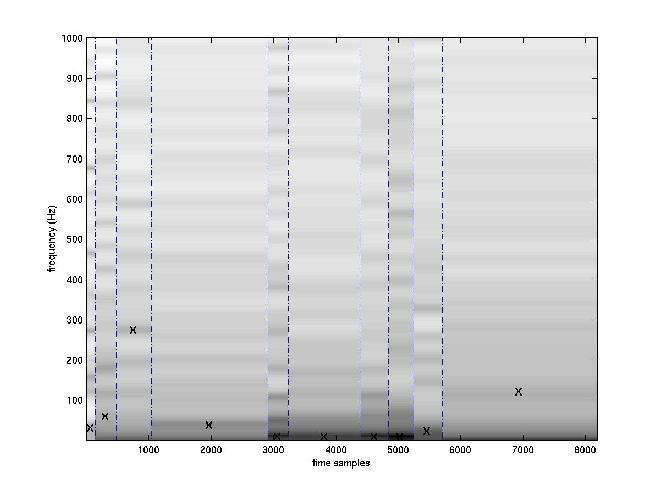
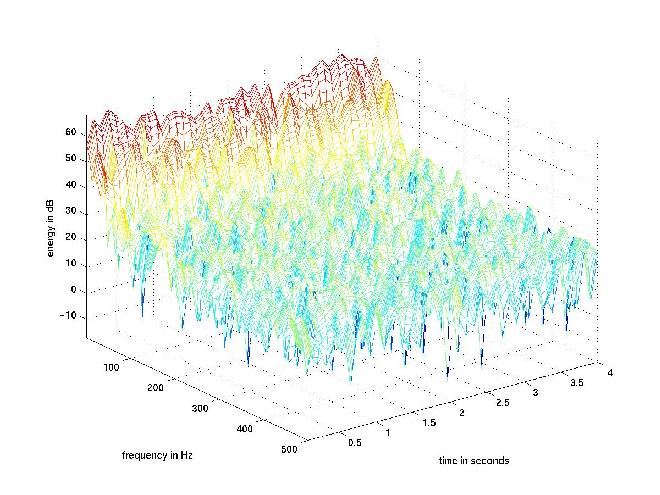 TFD of the MCI signal.
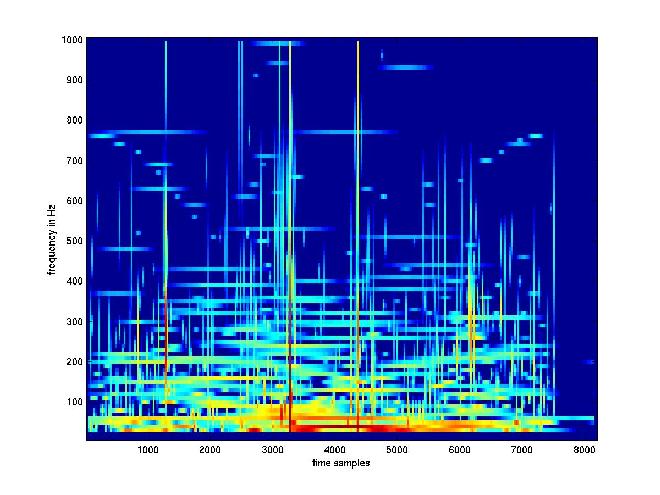
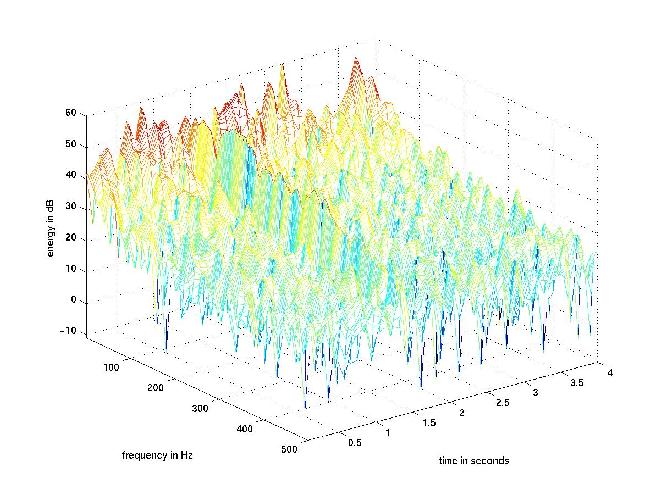 TFD of the MCI-filtered VAG signal. Note that the low-frequency MCI has been reduced. |
| Research Personnel |